


200
评论
查看更多
密码过期或已经不安全,请修改密码
修改密码
壹生身份认证协议书
同意
拒绝
同意
拒绝
同意
不同意并跳过





Stroke & Vascular Neurology(SVN)新近上线文章“Measures of intracranial compartments in acute intracerebral haemorrhage: data from the Rapid Intervention with Glyceryl Trinitrate in Hypertensive Stroke-2 Trial (RIGHT-2)”,来自英国诺丁汉大学Kailash Krishnan等。

脑出血量(Intracerebral haemorrhage volume, ICHV)对预后具有重要意义,作者团队应用CT扫描评估急性脑出血患者颅内腔室的测量,以及脑出血量(ICHV)/颅内容积(ICV)和脑出血量(ICHV)/脑实质体积(CPV)比值能否预测功能结局,还评估了脑池消失、中线移位、陈旧性梗死、脑白质疏松和脑萎缩是否与结局相关。
作者团队分析了来自RIGHT 2(Rapid Intervention with Glyceryl Trinitrate in Hypertensive Stroke-2 Trial)研究的133例参与者数据。测量包括ICHV(使用ABC/2)和ICV(XYZ/2)(独立观察)。ICHV、ICV和CPV(semiautomated segmentation, SAS)、萎缩(intercaudate distance, ICD; Sylvian fissure ratio, SFR)、中线移位、脑白质疏松和脑池消失(视觉评估)。评估这些测量对第4天死亡和第90天不良功能结局的影响(改良Rankin量表 mRS>3)。
研究结果显示,XYZ和SAS之间的ICV具有显著性差异:mean (SD) = 1357 (219) vs 1420 (196),mean difference (MD) 62 mL (p<0.001)。ABC/2与SAS之间的ICHV无显著性差异。通过SAS、CPV、ICD、SFR、脑白质疏松和脑池评分测量的ICV具有非常好的一致性(所有组内相关性,n=10:观察者间0.72~0.99,观察者内0.73~1.00)。ICHV/ICV和ICHV/CPV与第90天的mRS、第4天死亡和急性神经功能恶化显著相关(all p<0.05),与ICHV相似。基线时的中线移位和脑池消失与不良功能结局相关,但陈旧性梗死、脑白质疏松和脑萎缩与此无关。

Figure 1. Receiver operating characteristic (ROC) analysis for day 90 modified Rankin scale of >3, day 4 death and acute neurological deterioration. Similar area under the curves was observed for ICH volume (ICHV) (semiautomated segmentation and ABC/2), ICH volume/ICV ratio (semiautomated segmentation and ABC/XYZ) and ICH volume/CPV ratio (semiautomated segmentation). AUROC, area under the receiver operating characteristics curve; CPV, cerebral parenchymal volume; ICH, intracerebral haemorrhage; ICV, intracranial volume; SAS, semiautomated segmentation.
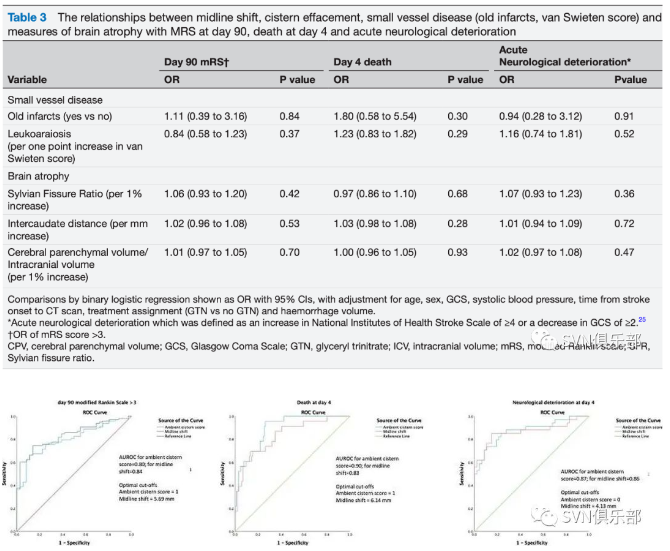
Figure 2. Receiver operating characteristic (ROC) analysis of ambient cistern score and midline shift for day 90 modified Rankin scale of >3, day 4 death and acute neurological deterioration. Ambient Cistern Score had slightly better accuracy than midline shift for prediction of day 4 death and neurological deterioration while midline shift was marginally better in predicting day 90 modified Rankin scale of >3. AUROC, area under the receiver operating characteristics curve.

Figure 3. Receiver operating characteristic (ROC) analysis of brain atrophy/small vessel disease markers for day 90 modified Rankin scale of >3, day 4 death and acute neurological deterioration. The addition of brain atrophy/small vessel disease markers to known prognostic factors (age, sex, onset to CT time, treatment with GTN, Glasgow Coma Scale, systolic blood pressure and ICH volume) did not improve the accuracy of outcome prediction. AUROC of models including these prognostic factors but without brain atrophy/small vessel disease markers=0.86, 0.85 and 0.85, respectively, for day 90 modified Rankin scale of >3, day 4 death and acute neurological deterioration, which was not very different from those with brain atrophy/small vessel disease markers. AUROC, area under the receiver operating characteristics curve; CPV, cerebral parenchymal volume; GTN, glyceryl trinitrate; ICH, intracerebral haemorrhage; ICV, intracranial volume.

Figure 4. Scatterplot showing predicted probabilities of haemorrhage expansion with increasing ICHV, ICHV/ICV and ICHV/CPV. The risk of haemorrhage expansion increased with larger ICH volumes but plateaued at 60 mL, when the risk is no longer significant. similar observations were seen with ICH volume/ICV and ICH volume/CPV ratios at cut-offs of >4%. *Models were adjusted for systolic blood pressure, time from stroke onset-to-CT scan and treatment with GTN. CPV, cerebral parenchymal volume; GTN, glyceryl trinitrate; ICHV, intracerebral haemorrhage volume; ICV, intracranial volume.
研究结论:颅内腔室测量和视觉估计是可重复的,针对ICH和CPV校正的ICHV可有助于预测急性卒中预后,中线移位和脑池消失的存在可预测结局,但其机制尚需在更大规模的研究中进行验证。

来源:SVN俱乐部
转载已获授权,其他账号转载请联系原账号
罕见病诊疗指南——抗 LGI1 抗体相关脑炎【神经系统罕见病】
《中国卒中学会关于无症状性颈动脉狭窄筛查的科学声明》在线发布
ISC 2022前沿速递|应用西洛他唑双联抗血小板治疗对卒中二级预防影响的性别差异
ISC 2022|续写新篇章 —— “替奈普酶”精彩继续……
血栓预防及血栓形成的治疗推荐丨2022 AHA/ASA自发性脑出血患者管理指南
院前和初始医疗系统的推荐丨2022 AHA/ASA自发性脑出血患者管理指南
Lancet:静脉溶栓替奈普酶(0.25 mg/kg) VS 阿替普酶
查看更多
 中国医学论坛报
中国医学论坛报 壹生
壹生 今日肿瘤
今日肿瘤 今日循环
今日循环 今日糖尿病
今日糖尿病 今日口腔
今日口腔 全科周刊
全科周刊 脱贫地区农副产品网络销售平台
脱贫地区农副产品网络销售平台
京公网安备 11010202008182号
| 互联网新闻信息服务许可证编号:10120190017